

Tabletop Puppets Acting Workshop for Adults at the Falmouth Public Library
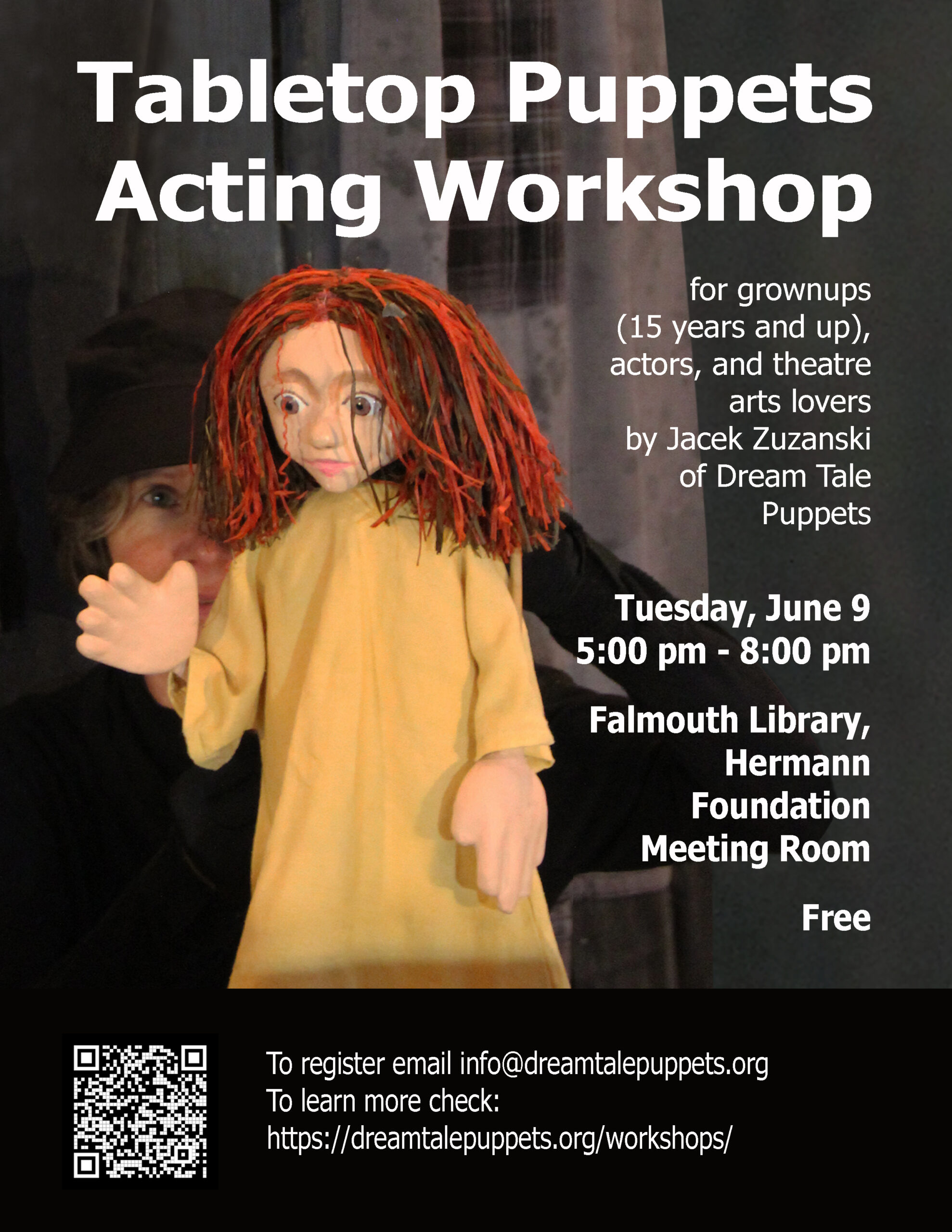
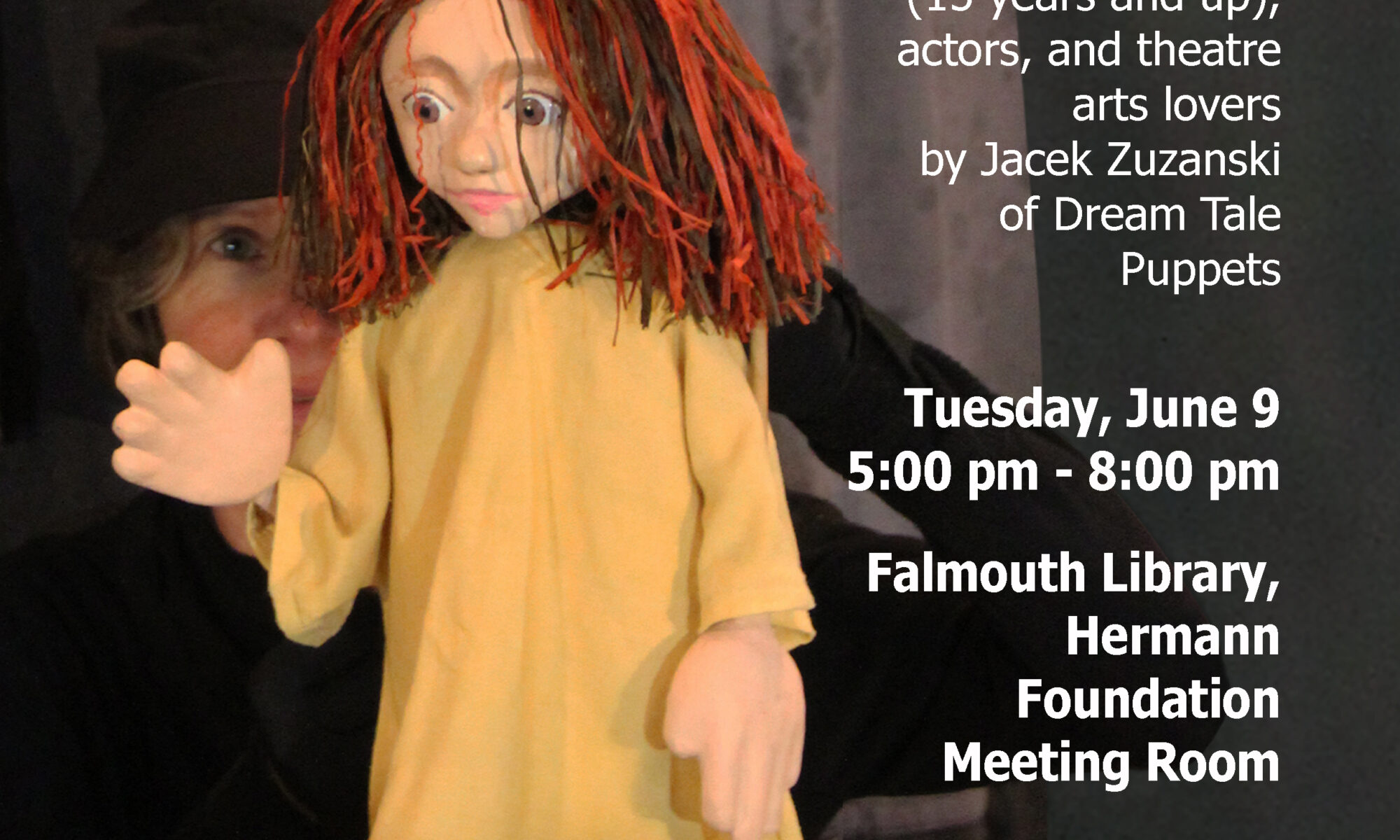
Jacek Zuzanski of Dream Tale Puppets invites actors and theatre arts lovers to the Tabletop Puppets Acting Workshop for grown-ups (15 years and up). The class will be offered at the Falmouth Public Library.
The workshop will introduce participants to the art of giving life to an object and turning it into a stage character. Participants will explore the expressive principles and acting techniques used in Dream Tale Puppets’ tabletop puppet performances. The experience may be especially interesting to actors, teachers, artists, and anyone who enjoys role-playing, fantasy, and creative self-expression. Puppets will be provided.
Jacek Zuzanski, trained professionally in acting, directing, and puppetry in Poland, has forty years of experience as an actor, teacher, designer, builder, and theatre director.
Participation is free, but space is limited. To register, please email Dream Tale Puppets’ or use the contact form on the website: https://dreamtalepuppets.org/
The project will be an abbreviated version of the previous workshop, described at the Dream Tale Puppets’ blog: https://dreamtalepuppets.org/2023/05/07/acting-with-tabletop-puppets/